
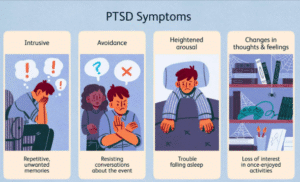
Post-Traumatic Stress Disorder (PTSD) is a psychiatric condition that can develop after a person experiences, witnesses, or learns about a traumatic event—such as violence, abuse, serious accidents, natural disasters, or life‑threatening medical emergencies—that threatens physical or emotional safety. PTSD is characterised by persistent, distressing symptoms that continue well beyond the initial shock: intrusive memories or flashbacks, avoidance of reminders, negative changes in thinking and mood, and increased arousal or reactivity. These symptoms are the result of the brain’s stress and memory systems becoming dysregulated after trauma, so daily tasks, relationships, work, sleep, and physical health can all be affected.
Not everyone exposed to trauma develops PTSD; risk depends on factors such as the intensity and duration of the trauma, prior mental health, early life stress, social support, and coping resources. Symptoms may appear immediately, weeks later, or even years after the event. Early recognition and treatment—using evidence‑based therapies like trauma‑focused CBT, EMDR, or somatic approaches—significantly improve recovery.
Understanding PTSD
PTSD is not a sign of weakness or personal failure. It reflects how the brain’s survival systems respond to overwhelming danger and then remain stuck in a heightened state of alert even after the threat has passed. Trauma can change how the brain processes fear, stores memories, and regulates emotions and behaviour. Three brain regions are especially involved:
Amygdala — the fear alarm
What it does: Detects threat and triggers fast emotional and bodily responses (fight, flight, freeze).
How trauma changes it: The amygdala can become hypersensitive and overreact to cues that resemble the original danger, even when those cues are safe.
Common effects: Intense fear, sudden panic, being easily startled, feeling constantly unsafe.
Everyday example: After a car crash, the sound of a horn or screeching brakes causes a surge of terror and physical symptoms (racing heart, sweating) as if the accident is happening again.
Practical note: Grounding techniques and breathing exercises can help reduce immediate amygdala-driven panic by engaging the body’s calming systems.
Hippocampus — the memory organizer
What it does: Encodes, organizes, and contextualizes memories; helps place events in time and separate past from present.
How trauma changes it: Stress hormones during trauma can disrupt how memories are formed and integrated, producing fragmented, overly vivid, or gap-filled recollections.
Common effects: Flashbacks that seem “live,” difficulty recalling the sequence of events, sensory fragments (smells, sounds) that trigger intense remembering.
Everyday example: Someone assaulted may vividly recall a particular smell or the click of a door but cannot retrieve a clear narrative of what happened before or after.
Practical note: Therapies that help reprocess and contextualize memories (e.g., EMDR, trauma-focused CBT) aim to restore hippocampal function so memories feel like past events rather than present threats.
Prefrontal cortex — the rational thinker and regulator
What it does: Supports decision-making, planning, impulse control, and down‑regulation of strong emotions; helps interpret safety signals.
How trauma changes it: The prefrontal cortex can become less effective at inhibiting the amygdala and organizing responses, reducing a person’s ability to calm themselves or reassess danger logically.
Common effects: Difficulty concentrating, impaired decision-making, emotional reactivity, trouble using reason to soothe fear.
Everyday example: After a medical emergency, a person may catastrophize small bodily sensations (fast heartbeat = another crisis) despite medical reassurance.
Practical note: Skills training from therapies (emotion regulation, cognitive restructuring, mindfulness) strengthens prefrontal control over fear-driven responses.
How these systems interact
When working normally, the prefrontal cortex helps the hippocampus and amygdala coordinate: memory places events in time, the prefrontal cortex evaluates current safety, and the amygdala responds proportionately. Trauma can dysregulate this balance: a hyperactive amygdala triggers fear, a fragmented hippocampus fails to contextualize memories, and a weakened prefrontal cortex cannot provide calm reassessment. The result is persistent, disproportionate fear and intrusive memories.
Risk and resilience factors
Not everyone who experiences trauma develops PTSD. Factors that increase risk include repeated or prolonged trauma, early-life adversity, lack of social support, prior mental-health conditions, and high trauma severity. Protective factors include strong social connections, timely support, adaptive coping skills, and early access to effective interventions.
Takeaway
PTSD is a brain-based response to overwhelming stress, not a personal shortcoming. Understanding which brain systems are involved helps explain why symptoms feel so vivid and why certain treatments (exposure, memory reprocessing, skills training) are effective. If intrusive memories, avoidance, mood changes, or hyperarousal are disrupting daily life, consult a mental-health professional for assessment and evidence-based treatment.
Why trauma responses affect thoughts, emotions, and the body
When the brain interprets an event as life‑threatening, it shifts into survival mode. That response—designed to protect you—recruits fast, automatic systems (fear, stress hormones, bodily arousal) that prioritize immediate safety over careful thinking. If those systems remain activated after the trauma, they change how you think, feel, and sense your body:
Thoughts (threat-focused thinking)
- The brain’s predictions shift toward danger: “Something bad will happen again,” “I’m not safe,” or “It’s my fault.”
- Reasoning and memory are biased by fear, so neutral information is more likely to be seen as risky.
- This thinking keeps you alert for threats but also fuels anxiety, avoidance, and negative self-beliefs.
Emotions (heightened or blunted)
- Emotions may swing between sudden fear, anger, guilt, or shame and emotional numbness or detachment.
- Numbness can be the brain’s attempt to reduce pain, while intense emotions are the alarm system still firing.
- Both patterns make it harder to connect with others, enjoy activities, or regulate mood.
Body (chronic arousal and physical symptoms)
- Stress systems release adrenaline and cortisol, producing a racing heart, sweating, tight muscles, breathlessness, stomach upset, and sleep disturbance.
- The nervous system becomes tuned to detect and respond to danger, so minor cues can trigger strong physical reactions.
- Over time, this ongoing arousal can worsen sleep, concentration, and physical health (fatigue, headaches, chronic pain).
Examples
Loud noises: After domestic violence, raised voices or sudden loud sounds may trigger jumpiness or panic because the brain associates noise volume with danger.
Avoiding roads: Someone who witnessed a serious crash may avoid highways, busier streets, or sitting next to windows—small safety choices that can gradually narrow daily life.
Emotional numbness: A trauma survivor might smile and interact normally but feel “empty” inside, disconnected from feelings and relationships.
Nightmares and flashbacks: A survivor of a fire may repeatedly dream of flames or smell smoke at random, waking in terror; sensory fragments become vivid reminders.
Safety behaviours: Following a burglary, checking locks several times, sleeping with lights on, or avoiding being alone may feel necessary but keep fear active.
Why these reactions persist and become problematic
- Short-term benefits, long-term cost: Avoidance and safety behaviours reduce fear in the moment but prevent the brain from relearning that the situation is now safe. That keeps the fear network active.
- Memory disruption: Fragmented trauma memories can feel like the event is happening now, not in the past, which fuels intrusions.
- Social impact: Isolation and misunderstood reactions strain relationships and reduce the social support that helps recovery.
What helps
Grounding and breathing: Simple grounding (5-4-3-2-1 sensory method) and slow abdominal breathing can calm the body during a surge of panic.
Gentle exposure: Gradual, safe facing of reminders (with a therapist) helps the brain update its sense of safety.
Social support: Talking to someone who listens without judgment reduces shame and isolation.
Professional care: Evidence‑based therapies (TF‑CBT, EMDR, exposure therapies, somatic approaches) address thinking patterns, memory processing, and bodily regulation.
In short
PTSD responses are the brain’s protective systems stuck in high gear. They affect thinking, emotions, and bodily sensations in ways that made sense during the trauma but cause harm afterward. With appropriate strategies and professional support, these systems can be retrained and symptoms reduced.

Core symptom: Intrusive memories
Intrusive memories are sudden, unwanted re-experiencings of the trauma that force the past into the present. They can be sensory (images, sounds, smells), emotional, or bodily, and they often arrive without warning. These experiences can make a person feel trapped, disoriented, or convinced the danger has returned.
Common intrusive symptoms
Flashbacks:
Vivid re-living of the traumatic event as if it is happening now. During a flashback, people may lose awareness of their current surroundings and respond with intense fear or defensive behaviour.
- Example: After a road crash, the sound of screeching brakes triggers a flashback—heart racing, crying, trembling, and an overwhelming sense of being back in the vehicle.
- Coping tip: If a flashback begins, use grounding: name five things you can see, four you can touch, three you can hear, two you can smell, and one you can taste; breathe slowly and tell yourself the event is in the past.
Nightmares and trauma-related dreams:
Recurrent, distressing dreams that replay the trauma or use symbolic content to evoke the same emotional response.
- Example: A fire survivor repeatedly wakes from dreams of smoke and flames, feeling panicked and sweating.
- Coping tip: Maintain sleep hygiene (regular bedtime, reduce screens before sleep), try a calming bedtime routine, and discuss frequent nightmares with a therapist who can use imagery rehearsal or trauma therapy techniques.
Intense physical or emotional reactions to reminders:
Strong bodily responses—racing heart, sweating, panic, shortness of breath—or sudden overwhelming emotions when encountering triggers (sounds, smells, places, people, or dates).
- Example: A survivor of emotional abuse feels breathless and panicky at the sound of shouting, even when the argument is unrelated.
- Coping tip: Practice slow diaphragmatic breathing (4–6 breaths per minute) and grounding. If reminders are frequent, consider working with a therapist on gradual, safe exposure to reduce reactivity.
Intrusive thoughts and images:
Unwanted, often vivid mental pictures, phrases, or memories that intrude during everyday activities and are hard to dismiss.
-
-
Example: Someone who witnessed violence suddenly imagines the scene while at work or commuting.
-
Coping tip: Label the thought as an intrusion (“That’s a trauma memory, not now”), gently refocus attention to the present task, or use brief mindfulness exercises to observe the thought without engaging it.
-
When intrusions become a problem
- Intrusions that are frequent, prolonged, or intensely distressing; that cause functional impairment (avoidance, missed work, relationship strain); or that include dissociative symptoms (loss of awareness, detachment) warrant professional assessment.
- Evidence-based treatments (TF‑CBT, EMDR, prolonged exposure) specifically target intrusive memories by helping the brain reprocess and contextualize the traumatic material so memories feel like past events rather than present threats.

What Triggers Intrusions?
Intrusions can be triggered by anything that resembles the traumatic event—even if it seems small or unrelated to others. Common triggers include:
- Sounds: sirens, shouting, loud noises
- Smells: smoke, perfume, hospital scents
- Dates or anniversaries: the day the trauma happened
- Visual cues: a similar car, building, or person
- Random moments: sometimes intrusions appear without a clear trigger
Example:
A person assaulted in a dark alley may experience a sudden flashback simply by walking past a dim street or hearing footsteps behind them.
Avoidance
In PTSD, the brain’s main goal becomes protecting you from anything that feels dangerous, even if those things are no longer harmful. To achieve this, the mind starts avoiding anything connected to the traumatic experience.
While avoidance may reduce stress in the moment, it prevents healing and often makes symptoms stronger over time.
Common Avoidance Signs
1. Avoiding People, Places, or Situations That Remind You of the Trauma
The person may change routines, skip important events, or stay away from anything that feels similar to the traumatic environment.
Examples:
- After a car crash, someone avoids highways or refuses to sit in a vehicle.
- A person who experienced workplace harassment may avoid the office or feel panic when passing by that area.
- Someone who survived domestic violence avoids crowded or loud places where they feel unsafe.
2. Refusing to Think or Talk About the Event
The mind blocks conversations, thoughts, or memories that feel too painful. This can look like shutting down emotionally or changing the topic instantly.
Examples:
- When someone asks what happened, the person says “I don’t want to talk about it,” or becomes visibly tense.
- They distract themselves with TV, mobile, or work whenever intrusive memories start coming back.
3. Emotional Numbness — Feeling Disconnected From Yourself or Others
To avoid feeling pain, the brain may shut down emotions altogether.
This detachment can look like coldness, lack of interest, or difficulty forming emotional bonds.
Examples:
- A person feels “blank” even during happy moments.
- They find it hard to express love, excitement, or sadness.
- Feel like they are watching life from a distance rather than living it.
4. Using Distractions, Work, or Sleep to Avoid Painful Feelings
People may keep themselves constantly busy or exhausted to avoid facing the trauma.
Examples:
- Working long hours to avoid being alone with thoughts.
- Sleeping excessively to escape emotional pain.
- Overuse of phone, social media, TV, or gaming to avoid thinking about the event.
- Excessive cleaning or overplanning as a way to stay mentally occupied.

Why avoidance makes PTSD worse over time
Avoidance gives fast relief: when you avoid a reminder, your anxiety drops immediately, so the brain learns that avoidance “works.” That short‑term success becomes a habit, but it blocks the deeper learning the brain needs to update its sense of safety. In other words, avoidance stops the memory and fear from being processed and integrated into a normal past event, so the fear remains active and unpredictable.
Longer‑term consequences
- Shrinking life: Avoidance narrows daily routines—fewer places visited, activities skipped, and opportunities missed—which reduces quality of life and can lead to depression.
- Relationship strain: When someone withdraws, hides symptoms, or refuses to discuss the trauma, friends and family may feel confused, shut out, or helpless, increasing isolation and conflict.
- Heightened anxiety: Because avoidance prevents relearning safety, the brain remains primed for threat. Triggers become broader and more sensitive, making everyday life feel more dangerous.
- Strengthened intrusive symptoms: Avoidance prevents emotional processing and meaning‑making. Intrusions (flashbacks, nightmares) remain vivid and frequent because the memory network remains unintegrated.
How healing happens
- Safe facing and processing: Recovery usually begins with gradual, supported exposure to reminders and structured processing of the traumatic memory. This teaches the brain that reminders are not the same as current danger.
- Skills + exposure: Learning grounding, emotion regulation, and cognitive strategies before and during exposure improves tolerance and reduces overwhelm.
- Professional support: Trauma-focused therapies (TF‑CBT, prolonged exposure, EMDR, or somatic approaches) provide a scaffolded, evidence‑based process for reducing avoidance and rebuilding function.
Practical next steps
- Notice and name avoidance (what you avoid, when, and why).
- Start with small, manageable exposures and pair them with calming skills.
- Rebuild social contact—invite a trusted person to join you in low-stress activities.
- Seek a trauma‑informed therapist for structured treatment when avoidance disrupts life.
Negative Changes in Thoughts & Mood
Trauma doesn’t just affect memories—it can also reshape the way a person sees themselves, other people, and the entire world. These changes can feel heavy, confusing, and deeply emotional. Many people with PTSD describe it as “carrying a weight they cannot explain.”
Common Signs of Negative Thought & Mood Changes
1. Persistent Sadness, Guilt, or Shame
These emotions often stay for a long time, even when the person logically knows they didn’t cause the trauma.
Examples:
- Feeling guilty for surviving when others didn’t (“Survivor’s guilt”).
- Blaming themselves for something they couldn’t control.
- Feeling ashamed about how they reacted during the traumatic event.
2. Feeling Emotionally “Flat” or Detached
The person may feel disconnected from their own emotions, relationships, or surroundings.
Examples:
- Not reacting emotionally to good or bad news.
- Feeling like life is happening “far away” or like they’re watching it from outside their body.
- Struggling to form or maintain emotional closeness with family or friends.
3. Loss of Interest in Activities Once Enjoyed
Things that previously brought happiness may no longer feel enjoyable or meaningful.
Examples:
- A person who loved music or art suddenly stops engaging with it.
- Someone who was social becomes withdrawn and avoids gatherings.
- Hobbies, sports, or work no longer feel motivating.
4. Negative Beliefs About Self, Others, or the World
Trauma can rewrite core beliefs, making the world feel unsafe.
Examples:
- “I am unsafe wherever I go.”
- “People cannot be trusted.”
- “I’m weak.”
- “It was my fault.”
- “Something bad will happen again.”
These beliefs may lead to constant fear, self-blame, or low self-worth.
5. Difficulty Experiencing Positive Emotions
Joy, love, or excitement may feel distant or completely absent.
Examples:
- Feeling unable to enjoy family time or celebrations.
- numbness feel even when something good happens.
- Having trouble expressing affection or happiness.
6. Memory Problems Related to the Trauma
Trauma affects how memories are formed and stored.
People may forget parts of the event or struggle with everyday concentration.
Examples:
- Not remembering important details of the trauma.
- Trouble focusing on conversations or tasks.
- Confusion about timelines (“I don’t remember what happened first”).
Impact on Relationships
These emotional and cognitive changes may cause the person to pull back from others—not because they don’t care, but because they feel too overwhelmed or disconnected.
This can lead to:
- Avoiding friends
- Feeling misunderstood
- Strained relationships
- Reduced communication
Understanding these symptoms helps reduce judgment and encourages compassionate support.
Increased Arousal & Reactivity
The nervous system stays on high alert, as if danger is still present.
Symptoms include:
- Irritability, sudden anger, or emotional outbursts
- Hypervigilance—constantly scanning for danger
- Sleep problems (insomnia, restless sleep)
- Difficulty concentrating
- Being easily startled
- Risky or self-destructive behavior in some cases
This “fight-or-flight mode” can be exhausting emotionally and physically.
Common Trauma Responses That Are Often Misunderstood
Many trauma responses are not always recognized as PTSD. These can include:
Emotional responses
- Feeling overwhelmed by small triggers
- Strong guilt or feeling responsible for the trauma
- Emotional numbness or detachment
Physical responses
- Chronic pain or fatigue
- Headaches, stomach issues
- Increased heart rate or breathlessness without medical cause
Behavioral responses
- Social withdrawal
- Misusing alcohol, food, or substances
- Overworking to avoid emotional pain

How PTSD affects daily life
PTSD can touch nearly every area of life, often in ways that are subtle at first and grow over time. Because symptoms can overlap with anxiety, depression, or anger, many people don’t realize PTSD is the underlying issue. Here are common domains affected, with everyday examples and brief actions to take.
Relationships
- What happens: Withdrawal, emotional numbness, irritability, trust difficulties, or over-reactivity to perceived threats can strain family, friendships, and romantic partnerships.
- Example: A partner avoids closeness or becomes easily angered during disagreements; friends feel shut out or unsure how to help.
- What to do: Communicate openly when possible, invite gentle conversations about needs, and consider couple or family therapy to rebuild connection.
Work or academics
- What happens: Concentration problems, memory gaps, avoidance of tasks or places, or sudden emotional reactions can reduce productivity and increase absenteeism.
- Example: A person misses deadlines after intrusive memories disrupt focus, or avoids returning to a workplace where harassment occurred.
- What to do: Use practical supports (task lists, timed work blocks), disclose to a trusted HR contact if safe, and seek workplace accommodations or phased return plans.
Sleep and physical health
- What happens: Nightmares, insomnia, hypervigilance, and chronic stress increase fatigue, weaken immunity, and worsen conditions like headaches, stomach problems, and chronic pain.
- Example: Frequent nightmares leave someone exhausted and less able to cope with daily stressors.
- What to do: Prioritize sleep hygiene, practice relaxation before bed, discuss medication or trauma-focused therapy with a clinician if sleep remains poor.
Decision‑making and concentration
- What happens: Heightened arousal and intrusive thoughts impair planning, problem-solving, and sustained attention.
- Example: Difficulty making routine decisions, forgetfulness, or poor concentration during meetings or classes.
- What to do: Break tasks into small steps, use reminders and checklists, and schedule demanding tasks during times of day when focus is better.
Self‑esteem and identity
- What happens: Trauma may produce shame, guilt, or beliefs like “I’m weak” or “I can’t trust myself,” which undermine self‑confidence and motivation.
- Example: Someone avoids trying new things for fear of failing or being retraumatized.
- What to do: Practice compassionate self-talk, keep a strengths list, and work with a therapist on cognitive restructuring to challenge unhelpful beliefs.
Overall sense of safety and future outlook
- What happens: The world can feel dangerous and unpredictable, leading to chronic worry, planning for worst-case scenarios, or withdrawing from future goals.
- Example: Avoiding travel, social events, or career moves because of fear something bad will happen.
- What to do: Gradually reintroduce valued activities with support, set small goals, and use grounding and reality-checking techniques to re-establish a sense of safety.
When to seek help
- If PTSD symptoms interfere with relationships, work/school, sleep, or daily functioning, or if you rely on substances or risky behaviour to cope, seek professional assessment.
- Early, trauma‑informed treatment improves outcomes. Evidence-based therapies reduce symptoms and help people reclaim daily life.
Quick practical tips
- Track one symptom that bothers you (sleep, concentration, avoidance) for a week to notice patterns.
- Create a short safety plan for high‑stress moments (who to call, grounding steps, safe place).
- Reach out to one trusted person and name one small support you need (a listening ear, help with chores, company for an appointment).
When to Seek Help
You should consider professional support if:
- Symptoms last longer than one month
- They disrupt work, relationships, or daily functioning
- You feel emotionally overwhelmed or unsafe
- Nightmares or flashbacks are frequent
- Avoidance is restricting your life
- You feel disconnected, numb, or unable to cope with daily stress
PTSD is highly treatable with the right help.
Therapies like CBT, EMDR, trauma-focused counselling, and mind–body approaches can help you regain safety and emotional balance.
👉 If you need guidance or wish to book a counselling session, reach out here:
Contact Us
Effective Treatments for PTSD
Several evidence-based therapies help individuals process trauma safely:
- Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
- EMDR (Eye Movement Desensitization and Reprocessing)
- Prolonged Exposure Therapy
- Somatic therapies (body-focused)
- Mindfulness-based therapies
- Medication when needed (under psychiatric guidance)
Early intervention often leads to better recovery.

How to Support Someone With PTSD
- Listen without judgment
- Avoid pushing them to “move on”
- Encourage professional help
- Be patient—healing is not linear
- Help create a safe, calm environment
Final Thoughts
PTSD is a real and treatable condition—not a weakness or moral failing. Trauma can leave the brain’s alarm systems locked on, producing distressing memories, avoidance, mood changes, and physical symptoms that make daily life harder. The good news is that the brain can relearn safety: evidence‑based therapies (TF‑CBT, EMDR, prolonged exposure), somatic approaches, medication when appropriate, and steady social support all help people process trauma, reduce symptoms, and rebuild meaning and connection.
If you or someone you care about is struggling with intrusive memories, strong avoidance, emotional numbness, or constant hypervigilance, reaching out for professional assessment is an important first step. Small, practical actions—using grounding and breathing techniques, reconnecting with trusted people, and seeking a trauma‑informed therapist—can make a meaningful difference. Recovery is a process, often non‑linear, but with the right care and support most people regain stability, safety, and hope.
Frequently Asked Questions (FAQs)
1. What is Post-Traumatic Stress Disorder (PTSD)?
PTSD is a mental health condition that develops after experiencing or witnessing a traumatic event.
2. What are the main symptoms of PTSD?
Symptoms include flashbacks, nightmares, avoidance, emotional numbness, and hypervigilance.
3. Can PTSD develop months after trauma?
Yes, PTSD symptoms can appear weeks, months, or even years after the traumatic event.
4. What causes PTSD?
PTSD is caused by trauma affecting brain areas like the amygdala, hippocampus, and prefrontal cortex.
5. Is PTSD treatable?
Yes, PTSD is highly treatable with therapy, medication, and coping strategies.
6. What triggers PTSD symptoms?
Triggers include sounds, smells, places, memories, or situations linked to the trauma.
7. Can PTSD affect physical health?
Yes, it can cause headaches, fatigue, stomach problems, and increased heart rate.
8. What is the best treatment for PTSD?
Treatments include CBT, EMDR, exposure therapy, and mindfulness-based approaches.
9. When should I seek help for PTSD?
If symptoms last more than a month or affect daily life, professional help is recommended.
10. Can PTSD go away on its own?
Some symptoms may improve, but most people benefit from structured therapy and support.
References
- American Psychiatric Association (DSM-5)
https://www.psychiatry.org/psychiatrists/practice/dsm - National Institute of Mental Health (NIMH) – PTSD
https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd - World Health Organization (WHO) – ICD-11
https://icd.who.int/en - Monoprova Counselling
https://monoprovacounselling.in/about-us/ - Contact / Book Appointment
https://monoprovacounselling.in/contact/
This article is written for knowledge purposes, aiming to help readers understand the topic better and gain useful insights for learning and awareness.
Pingback: Why Your Mind Creates Problems Even When Everything Is Fine