

Could an arthritis drug relieve depression? New trial finds IL‑6 blockade may help treatment‑resistant depression.
Introduction:
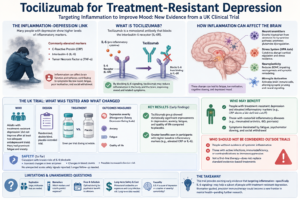
Treatment‑resistant depression (TRD) affects about 20–30% of people with major depressive disorder (MDD). For them, standard antidepressants and psychotherapy fall short, leaving persistent symptoms, impaired functioning, and higher suicide risk. That pressing need has pushed researchers beyond traditional targets toward novel biological approaches—ketamine and neuromodulation among them—and, increasingly, toward the immune system.
Over the past decade, evidence has mounted linking systemic inflammation and depressive symptoms. People with depression often show elevated markers such as C‑reactive protein (CRP), interleukin‑6 (IL‑6), and tumor necrosis factor alpha (TNF‑α). Patients with inflammatory illnesses—rheumatoid arthritis, psoriasis, inflammatory bowel disease—carry higher rates of depression, and inflammatory events (infections or cytokine therapies) can trigger depressive syndromes. Those observations underpin a testable idea: for a subset of people, inflammation contributes to depression—and reducing inflammation might improve mood.
What is tocilizumab and why IL‑6?
Tocilizumab is a monoclonal antibody that blocks the interleukin‑6 receptor (IL‑6R). Clinically, it treats conditions driven by IL‑6–mediated inflammation, including rheumatoid arthritis and cytokine release syndrome. IL‑6 itself is a pro‑inflammatory cytokine frequently elevated in people with depression. It influences brain function by crossing—or signaling across—the blood‑brain barrier, activating microglia and astrocytes, altering neurotransmitter metabolism, and reducing neuroplasticity. IL‑6 also contributes to “sickness behavior”: fatigue, social withdrawal, reduced motivation—symptoms resembling depression.
The UK tocilizumab trial: what was tested and what changed
Researchers in the UK ran a randomized, placebo‑controlled trial of tocilizumab in adults with treatment‑resistant depression—people who had not improved after at least two adequate antidepressant trials. The trial enrolled participants presenting with prominent depressive symptoms often accompanied by fatigue and anxiety.
Participants received tocilizumab (per the trial dosing schedule) or placebo, and outcomes were assessed using standard depression scales (for example, the Montgomery‑Åsberg Depression Rating Scale) alongside measures of anxiety, fatigue, and quality of life. Early results reported statistically significant improvements in depression severity, anxiety, fatigue, and overall quality of life in the tocilizumab group versus placebo. Benefits were larger in those with higher baseline inflammatory markers (e.g., elevated CRP or IL‑6), suggesting a biomarker‑driven response.
Safety findings aligned with known risks of IL‑6 blockade—transient changes in liver enzymes and blood counts, and a theoretical increased risk of infection—but the trial did not report unexpected acute safety signals. Longer follow‑up will be essential to understand long‑term immunologic consequences.
Why these early results matter
These findings translate the inflammation‑depression hypothesis into clinical testing and offer a plausible precision‑medicine pathway: identify biomarker‑positive patients whose depressive symptoms may be driven, at least in part, by inflammation and treat them with targeted immunotherapy. They fit an emerging pattern across multiple studies: anti‑inflammatory treatments often show the strongest antidepressant effects in people with elevated baseline inflammation.
Mechanisms in plain language
Inflammation likely impacts mood through several interacting pathways:
- Neurotransmitters: Inflammation activates enzymes that divert tryptophan away from serotonin production toward kynurenine metabolites. Some kynurenine products are neuroactive and may promote glutamate dysregulation.
- Stress system: Cytokines can dysregulate the hypothalamic‑pituitary‑adrenal (HPA) axis, altering cortisol responses and stress resilience.
- Neuroplasticity: Cytokines reduce neurotrophic factors such as BDNF, impairing neurogenesis and synaptic remodeling in mood‑relevant regions like the hippocampus.
- Microglia: Peripheral cytokines can activate brain immune cells, changing synaptic pruning and neural signaling.
Together, these changes can produce fatigue, low motivation, cognitive slowing, and mood disturbance—the behavioral signature of sickness and, in some cases, depressive illness.
Who may benefit — and who shouldn’t (yet)
Potentially appropriate candidates:
- People with TRD who show elevated inflammatory markers (for example, CRP above a lab‑defined cutoff).
- Patients with comorbid inflammatory diseases where cytokine blockade treats both conditions.
- Individuals whose symptoms are dominated by fatigue, psychomotor slowing, and social withdrawal.
Who should not be considered outside trials:
- People without evidence of systemic inflammation—broad application is unsupported.
- Those with active infections, immunodeficiency, or medical contraindications to immunosuppression.
- Patients seeking first‑line therapy—immunotherapy is not a substitute for standard evidence‑based initial treatments.
Limitations and unanswered questions
Caution is warranted. The reported results are early and may come from a limited sample size or interim analysis. Key questions remain:
- Replication: Larger, multicenter trials are needed to confirm efficacy and safety.
- Biomarker thresholds: Which inflammatory markers and cutoffs best predict response?
- Dose and schedule: The optimal dosing regimen for psychiatric benefit may differ from rheumatologic practice.
- Long‑term safety and cost: Monoclonal antibodies are expensive and carry infection risk. Longitudinal data are essential.
- Causality: Elevated IL‑6 may be a marker of severity or comorbid illness rather than a causal driver of mood. Mechanistic studies should accompany clinical trials to clarify causal pathways.
Practical advice for clinicians and patients
- Awareness: Clinicians should recognize inflammation as a potential contributor to depression and consider measuring CRP or other markers in treatment‑resistant cases.
- Trials first: Interested patients should be referred to clinical trials rather than seeking off‑label immunosuppression outside research settings.
- Risk–benefit: Any consideration of immunotherapy must balance psychiatric benefits against infection risk, liver effects, and cost.
- Holistic care: Immunotherapy, if effective for a given patient, would likely complement—not replace—psychotherapy, psychosocial supports, and other evidence‑based treatments.
Illustrative vignette
A 45‑year‑old with TRD and an elevated CRP (7 mg/L) suffers severe fatigue, anhedonia, and cognitive slowing. After joining a controlled trial of tocilizumab, she reports gradual improvement in energy and mood over weeks, matched by reductions in inflammatory markers—an outcome consistent with the hypothesized biomarker‑driven response, though anecdotal and needing confirmation in larger samples.
Broader implications
If subsequent trials confirm benefit, IL‑6 blockade could become part of a precision psychiatry toolkit, offering a targeted option for biomarker‑positive TRD. It would also strengthen the case for integrated care that treats psychiatric symptoms alongside systemic inflammation. Policymakers and clinicians would need to weigh clinical benefit against cost and population‑level safety, and to develop clear guidelines for patient selection.
Calls to action
- For clinicians: Consider measuring CRP in TRD and refer eligible patients to trials.
- For patients: Talk to your psychiatrist before pursuing experimental treatments; ask about clinical trial opportunities.
Conclusion
Tocilizumab’s early promise in treatment‑resistant depression offers an intriguing precision‑medicine path linking inflammation to mood — but larger, longer trials and careful safety, cost, and biomarker work are essential before this approach becomes routine.
FAQ
Q: Is tocilizumab now a standard depression treatment?
A: No. Results are promising but preliminary. Tocilizumab is not standard care for depression outside research.
Q: Should I get my CRP tested for depression?
A: Discuss with your clinician. In TRD, measuring inflammatory markers can inform further evaluation and possible trial eligibility.
Q: Are there safer anti‑inflammatory options for depression?
A: Trials of NSAIDs, minocycline, and cytokine antagonists have mixed results; benefits tend to cluster in patients with elevated inflammation. Safer, cheaper options require more evidence.
References
Foley, É. M., Turner, N., Margelyte, R., et al. (2026). Interleukin‑6 as a treatment target for depression: A proof‑of‑concept randomized clinical trial. JAMA Psychiatry. Advance online publication. https://jamanetwork.com/journals/jamapsychiatry
University of Bristol. (2026, May 19). Pilot trial suggests anti‑inflammatory drug could help difficult‑to‑treat depression. https://www.bristol.ac.uk/news/2026/may/pilot-trial-suggests-anti.html
The Guardian. (2026, May 20). Immunotherapy could be used to treat depression, early trial suggests. https://www.theguardian.com/society/2026/may/20/immunotherapy-drug-tocilizumab-potential-treatment-depression-uk-trial
Foley, É. M., et al. (2024). The INSIGHT study: A randomised controlled trial of single‑dose tocilizumab in patients with depression and evidence of low‑grade inflammation. Psychological Medicine, 54(12), e212. https://doi.org/10.1017/S0033291724002128
FirstWord Pharma. (2026, May 21). Pilot trial suggests anti‑inflammatory drug could help difficult‑to‑treat depression. https://firstwordpharma.com/story/7458668
Neuroscience News. (2026, May 19). Arthritis drug rescues hard‑to‑treat depression. https://neurosciencenews.com/immunotherapy-arthritis-il6-depression-30735/
Doi, K., et al. (2024). Tocilizumab lowered risk of depression in patients with rheumatoid arthritis: A propensity‑score‑matched cohort study. Clinical Epidemiology, 16, 1345–1353. https://doi.org/10.2147/CLEP.S437878
Diniz, A. R., et al. (2018). Protocol for the INSIGHT study: A randomised controlled trial of single‑dose tocilizumab in patients with depression and evidence of low‑grade inflammation. BMJ Open, 8(9), e023177. https://doi.org/10.1136/bmjopen-2018-023177
Monoprova Counselling, (2026), “About Us”, Available at https://monoprovacounselling.in/ [Accessed on 18th May 2026]
This article is written for knowledge purposes, aiming to help readers understand the topic better and gain useful insights for learning and awareness.