

Beck’s cognitive therapy (CT) is the evidence-based treatment for depression, anxiety, PTSD, and more — and it works by fixing the one thing that drives all of them: your thoughts. If you’ve ever felt stuck in loops of worry, hopelessness, or self-criticism, CT might be the missing tool in your self-help toolkit.
Introduction
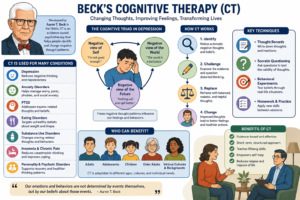
Aaron T. Beck’s cognitive therapy (CT) emerged in the 1960s from clinical observations of depressed patients and a research program that identified pervasive negative automatic thoughts and underlying dysfunctional beliefs (schemas) as central to emotional disorders. CT is a structured, time-limited, present-focused psychotherapy that targets cognition (thoughts, beliefs, assumptions) to produce emotional and behavioral change. The question “for which patients is Beck’s cognitive therapy used?” therefore requires both a description of the diagnostic groups where CT is first-line or evidence-based and an account of how the model is adapted by clinical presentation, severity, comorbidity, and treatment goals.
Core clinical populations
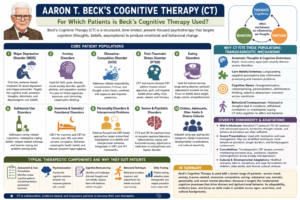
- Major depressive disorder (MDD): CT was originally developed from research with depressed patients and remains a first-line, evidence-based treatment for acute depression and relapse prevention. The therapy targets the cognitive triad (negative views of self, world, future), automatic thoughts, cognitive distortions, and depressogenic core beliefs or schemas. CT is effective both alone and as an adjunct to pharmacotherapy for moderate-to-severe depressive episodes.
- Anxiety disorders: CT/CBT protocols are widely used for generalized anxiety disorder (GAD), panic disorder, social anxiety disorder (social phobia), specific phobias, and separation anxiety (in youth). Treatment emphasizes cognitive restructuring of threat-related appraisals, exposure-based behavioral experiments, and correction of intolerance-of-uncertainty and catastrophic thinking patterns.
-
Obsessive–compulsive disorder (OCD):
Cognitive techniques (to address inflated responsibility, overestimation of threat, and thought–action fusion) are combined with behavioral exposure and response prevention; CT principles are integral to evidence-based OCD treatments.
- Post-traumatic stress disorder (PTSD): Cognitive processing therapy (CPT) and trauma-focused CBT adapt Beck’s cognitive model to target trauma-related appraisals, guilt, and negative beliefs about safety, trust, power, esteem, and intimacy. Cognitive re-evaluation and memory processing reduce intrusive symptoms and avoidance.
- Eating disorders: CT-based approaches (CBT-E, etc.) are used for bulimia nervosa, binge-eating disorder, and to some extent anorexia nervosa (with adaptations). They focus on dysfunctional beliefs about weight, shape, control, and perfectionism, plus behavioral strategies to normalize eating.
- Substance use disorders: Cognitive–behavioral approaches derived from Beck’s model are used to treat substance misuse by addressing craving-related cognitions, maladaptive coping beliefs, relapse-related schemas, and by teaching coping and problem-solving skills.
- Insomnia and somatic/functional disorders: CBT for insomnia (CBT-I) and cognitive–behavioral treatments for chronic pain, irritable bowel syndrome, and other somatic complaints use cognitive techniques to reframe catastrophic health beliefs and reduce symptom-related hypervigilance.
- Personality disorders and interpersonal problems: Schema-focused adaptations (schema therapy) and CBT-based treatments address entrenched maladaptive core beliefs and interpersonal schemas; CT is also integrated into dialectical or interpersonal frameworks for borderline and other personality disorders.
- Severe and psychotic disorders: Recovery-oriented cognitive therapy (CT-R) and CBT for psychosis adapt the cognitive model to focus on functional recovery, symptom appraisal (delusions, hallucinations), and coping strategies; CT can be adjunctive to medication for schizophrenia and bipolar disorder.
Why CT fits these populations: transdiagnostic mechanisms
- Automatic thoughts and cognitive distortions: Across disorders, patients report rapid, involuntary appraisals (automatic thoughts) that amplify distress—this is a central target in CT.
- Core beliefs/schemas: Longstanding negative assumptions (e.g., “I am unlovable,” “The world is dangerous,” “I must be perfect”) bias information processing and maintain maladaptive emotion and behavior across diagnostic categories.
- Cognitive biases: Overgeneralization, catastrophizing, personalization, dichotomous thinking, and selective abstraction function across depression, anxiety, and other disorders; CT teaches patients to identify and correct these biases.
- Behavioral consequences: CT links cognition to affect and behavior—maladaptive thoughts lead to avoidance, withdrawal, rumination, or maladaptive coping, so behavioral experiments, activity scheduling, and exposure are integrated.
Severity, comorbidity, and adaptations
- Mild-to-moderate presentations: Standard CT protocols (12–20 sessions) are often sufficient and cost-effective; structured sessions, homework, thought records, and behavioral activation are core components.
- Severe presentations: For severe depression, psychosis, or bipolar disorder, CT may be used alongside medication and case management, with modifications such as simplified cognitive techniques, more emphasis on behavioral activation, longer duration, and involvement of family or support networks.
- Comorbidities: When anxiety and depression co-occur, CT is adapted to simultaneously address both—transdiagnostic CBT protocols focus on core maintaining processes like avoidance and negative metacognitions.
- Cultural and developmental adaptations: CT has been adapted for children and adolescents (using age-appropriate metaphors, family involvement, and skills training), older adults (addressing bereavement and retirement issues), and different cultural contexts (modifying examples, idioms, and explanatory models).
Typical therapeutic components and why they suit certain patients
- Assessment and case formulation: CT uses a collaborative empirically based case formulation that links precipitating events, activating situations, automatic thoughts, mood/behavior, and underlying schemas; this helps align therapy to patient-specific problems and is especially helpful for complex or comorbid presentations.
- Psychoeducation: Patients learn the cognitive model (how thoughts influence feelings and behavior), which is useful for disorders where symptom misattribution or stigma reduces engagement (e.g., somatic symptom disorders).
- Cognitive restructuring: Socratic questioning, evidence gathering, and cost–benefit analysis are useful for patients with ruminative or worry-based conditions (depression, GAD).
- Behavioral experiments and exposure: Patients with avoidance-driven problems (phobias, PTSD, social anxiety) benefit from behavioral exposure; those with depression benefit from behavioral activation to combat inertia and anhedonia.
- Skills training: Problem-solving, assertiveness, and emotion regulation techniques help patients with interpersonal difficulties and personality disorder traits.
- Relapse prevention and maintenance: CT’s emphasis on identifying and modifying core beliefs supports long-term relapse prevention, which is particularly important in recurrent depression and chronic anxiety disorders.
Contraindications and considerations
- Cognitive capacity and acute risk: Patients with severe cognitive impairment, active psychosis without stabilization, or imminent suicide risk require careful triage, stabilization, and, often, adjunctive medical management before standard CT can proceed.
- Motivation and readiness: CT requires active participation and homework; patients low in motivation or with severe avoidance may need motivational enhancement, more behavioral focus, or adjunctive supportive interventions.
- Cultural fit: Therapists should adapt metaphors, idioms, and goals to align with patients’ cultural values; in some contexts, a purely cognitive approach may need integration with culturally congruent healing practices or family-based care.
Evidence base summary (what research shows)
- Depression: Numerous randomized controlled trials and meta-analyses show CT is effective for acute depression and reduces relapse rates compared with pharmacotherapy alone in many studies.
- Anxiety disorders: CBT protocols incorporating cognitive therapy principles demonstrate strong efficacy for panic disorder, social anxiety disorder, GAD, and specific phobias.
- OCD and PTSD: Cognitive approaches combined with behavioral interventions are first-line treatments for OCD and trauma-related disorders.
- Severe mental illness: Recovery-oriented cognitive therapies and adapted CBT show benefit as adjuncts for schizophrenia and bipolar disorder in improving functioning and reducing symptoms when used with medication.
These empirical findings explain why clinicians widely use CT across so many diagnostic groups and why treatment guidelines often list CBT/CT as recommended therapies.
Case examples (illustrative, condensed)
- Depression: A 35-year-old with recurrent MDD shows pervasive hopelessness and automatic thoughts like “I’m worthless.” CT uses activity scheduling to increase reinforcement, thought records to test negative predictions, and schema work to modify core beliefs; over sessions the patient’s activity and mood improve, and relapse prevention tools are taught.
- Social anxiety: A college student avoids speaking in class because of fear of negative evaluation. CT combines cognitive restructuring of catastrophic predictions with graded exposure (speaking tasks) and behavioral experiments; as predictive errors accumulate, anxiety decreases and social functioning improves.
- Chronic pain: A patient with fibromyalgia catastrophizes pain as a sign of worsening disease and avoids activity. CBT targets catastrophizing, encourages graded activity, and shifts pain-related beliefs—improving coping, reducing disability, and enhancing quality of life.
Practical guidance for clinicians
- Start with a clear, collaborative case formulation linking symptoms to thoughts, behaviors, and schemas.
- Match technique emphasis to presenting problems: prioritize behavioral activation for depression, exposures for avoidance-based anxiety, and cognitive restructuring for pervasive maladaptive beliefs.
- Use measurement-based care: baseline symptom scales (PHQ-9, GAD-7, PCL-5) guide progress monitoring and treatment adjustments.
- Integrate with other services when necessary: pharmacotherapy, family therapy, or vocational rehabilitation may be essential in complex or severe cases.
Common psychological terms used in CT (brief glossary)
- Automatic thoughts: Rapid, involuntary appraisals that arise in response to events and influence mood.
- Cognitive distortions: Systematic errors in thinking (e.g., catastrophizing, all-or-nothing thinking, personalization).
- Core beliefs/schemas: Deep, relatively stable rules or assumptions about self, world, and others that shape interpretations.
- Behavioral activation: Scheduling and increasing value-driven activities to counter withdrawal and inactivity.
- Exposure/behavioral experiment: Planned contact with feared stimuli or testing of predictions to disconfirm threat appraisals.
- Socratic questioning: A guided discovery technique where therapists ask targeted questions to help patients evaluate evidence and alternatives.
Conclusion
Beck’s cognitive therapy is broadly applicable across mood, anxiety, trauma-related, eating, and some severe mental disorders because many psychopathologies share cognitive mechanisms—automatic thoughts, cognitive distortions, and maladaptive schemas—that are directly targeted by CT interventions. With appropriate adaptations for severity, comorbidity, developmental stage, and cultural context, CT is a first-line or evidence-based option for a wide range of patients seeking psychological treatment.
Illustration/example:
Example thought-record entry: Situation—“I presented at work”; Automatic thought—“I sounded stupid”; Evidence for—“I stumbled once”; Evidence against—“Team later asked follow-up questions”; Alternative balanced thought—“I had one stumble, but overall my message was understood.”
FAQ
1. What is Aaron T. Beck’s cognitive therapy?
Aaron T. Beck’s cognitive therapy (CT) is a structured, time‑limited psychotherapy that focuses on the relationship between thoughts, emotions, and behaviors. It is based on the cognitive model, which holds that how a person interprets situations (their appraisals, automatic thoughts, and underlying core beliefs) strongly influences their emotional and behavioral reactions. Therapists help patients identify automatic thoughts, cognitive distortions (e.g., catastrophizing, overgeneralization), and maladaptive schemas, then guide them to test and reframe these cognitions using empirical evidence. CT is now a core component of cognitive–behavioral therapy (CBT) and is widely used in clinical practice.
2. Which patients benefit most from Beck’s cognitive therapy?
Beck’s cognitive therapy is evidence‑based for patients with a broad range of affective and anxiety disorders, including major depressive disorder, generalized anxiety disorder, panic disorder, social anxiety disorder, post‑traumatic stress disorder (PTSD), and obsessive–compulsive disorder (OCD). It is also effective for some eating disorders (such as bulimia nervosa and binge‑eating disorder), insomnia, chronic pain, substance use problems, and even schizophrenia and bipolar disorder when used as an adjunct to medication and other supports. The therapy works best for patients who are able to engage in self‑reflection, homework, and collaborative exploration of their thinking patterns.
3. Can CT be used for people with severe or persistent mental illness?
Yes, CT can be adapted for more severe or chronic conditions. For example, recovery‑oriented cognitive therapy (CT‑R) modifies Beck’s model for schizophrenia and related psychotic disorders, focusing on improving functioning, reducing distress about symptoms, and building a sense of agency. In bipolar disorder, CT helps patients manage mood‑related cognitions, detect early warning signs of relapse, and reduce behavioral risk‑taking. In these contexts, CT typically runs alongside pharmacotherapy, case management, and sometimes family‑based interventions, emphasizing goal‑oriented, problem‑solving strategies and relapse prevention rather than only symptom reduction.
4. Is cognitive therapy mainly for depression or can it treat anxiety too?
Cognitive therapy was initially developed from Beck’s work on depression, but it is now a first‑line treatment for many anxiety disorders as well. For generalized anxiety disorder (GAD), CT targets worry chains, intolerance‑of‑uncertainty, and safety‑seeking behaviors. Panic disorder, therapists help patients reinterpret bodily sensations (e.g., “I’m having a heart attack” → “This is anxiety”) and test predictions through behavioral experiments and exposure. For social anxiety and specific phobias, CT combines cognitive restructuring with graded exposure to feared situations, helping patients disconfirm catastrophic beliefs and reduce avoidance. In each case, the core mechanism is the modification of threat‑related appraisals and maladaptive assumptions.
5. How does cognitive therapy help PTSD patients?
For post‑traumatic stress disorder, CT (often in the form of cognitive processing therapy or trauma‑focused CBT) addresses trauma‑related cognitive distortions and negative beliefs about safety, trust, power, esteem, and intimacy. Patients learn to distinguish between what actually happened, what they came to believe about it, and how those beliefs affect their current emotions and behaviors. Therapists use Socratic questioning, written accounts of the trauma, and re‑evaluation of evidence to help patients revise self‑blame, guilt, or perception of permanent danger. Over time, this reduces intrusive memories, avoidance, and emotional numbing, supporting psychological recovery rather than only symptom suppression.
6. Can children and adolescents receive Beck’s cognitive therapy?
Yes, Beck’s model has been adapted for developmental contexts. Cognitive–behavioral interventions for children and adolescents use age‑appropriate language, metaphors, and concrete activities (e.g., drawings, games, behavioral experiments) to teach young people how thoughts influence feelings and actions. These adaptations are effective for pediatric depression, anxiety disorders, OCD, and school‑related problems such as low self‑esteem or social difficulty. Parental involvement, psychoeducation, and collaboration with teachers are often integrated so that caregivers can reinforce cognitive‑behavioral skills outside therapy sessions.
7. Does cognitive therapy work if someone has both anxiety and depression?
Cognitive therapy is well suited for comorbid anxiety and depression because both disorders share transdiagnostic processes such as rumination, catastrophic thinking, low self‑worth, and avoidance. In such cases, therapists may use a brief, transdiagnostic CBT protocol that targets core maintaining mechanisms (e.g., intolerance‑of‑uncertainty, behavioral withdrawal, negative core beliefs) rather than focusing narrowly on one diagnosis. Patients learn to recognize clusters of automatic thoughts (“I can’t cope”), test them empirically, and gradually increase engagement in activities that build mastery and pleasure, which improves both mood and anxiety over time.
8. Are there situations where cognitive therapy may not be the first choice?
Cognitive therapy is less suitable as a first‑line standalone treatment when patients are acutely psychotic, severely cognitively impaired, or in imminent danger of self‑harm without a stable support system. In these situations, stabilization (e.g., medication, crisis intervention, hospitalization) usually comes first. Therapists may also avoid purely cognitive approaches with patients who lack insight, have very low motivation, or cannot tolerate structured, homework‑based work. In such cases, CT may be introduced later or blended with supportive therapy, motivational interviewing, or other approaches that first build rapport, safety, and engagement.
9. How long does cognitive therapy usually last?
Cognitive therapy is typically time‑limited, often ranging from about 8 to 20 sessions for mild‑to‑moderate depression or anxiety, though some complex or chronic cases may require more. Sessions are usually weekly or biweekly, last about 45–60 minutes, and follow a structured format that includes setting an agenda, reviewing homework, working on target problems, and assigning new tasks. The brevity of CT is one reason it is recommended in many treatment guidelines; however, booster sessions or maintenance plans are often used to consolidate gains and prevent relapse, especially in recurrent depression.
10. What psychological skills do patients learn in cognitive therapy?
Patients in cognitive therapy become active “scientists” of their own thinking, learning several key skills grounded in cognitive and behavioral theory. They learn to identify automatic thoughts and core beliefs, detect cognitive distortions (e.g., all‑or‑nothing thinking, emotional reasoning), and use evidence‑based questioning to generate more balanced alternatives. They practice behavioral activation (scheduling meaningful activities), exposure to feared situations, and problem‑solving for real‑life stressors. Beyond symptom reduction, these skills build metacognitive awareness, emotional regulation, and self‑efficacy, which can help patients manage future stressors and reduce the risk of future episodes.
Reference
American Psychological Association. (2017). What is cognitive behavioral therapy? https://www.apa.org/ptsd-guideline/patients-and-families/cognitive-behavioral
Beck Institute for Cognitive Behavior Therapy. (2025). Understanding CBT. Beck Institute | Understanding CBT | Beck Institute
Cleveland Clinic. (2020). Cognitive behavioral therapy (CBT): What it is & techniques. Cognitive Behavioral Therapy (CBT): What It Is & Techniques
Mayo Clinic. (2025). Cognitive behavioral therapy. https://www.mayoclinic.org/tests-procedures/cognitive-behavioral-therapy/about/pac-20384610
National Institute for Health and Care Research. (2025). In brief: Cognitive behavioral therapy (CBT). National Health Service. https://www.ncbi.nlm.nih.gov/books/NBK279297/
National Center for Biotechnology Information. (2023). Cognitive behavior therapy. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK470241/
MonprovaHealing (2026), “About Us”, Available at https://monoprovacounselling.in/ [Accessed on 4th may]
This article is written for knowledge purposes, aiming to help readers understand the topic better and gain useful insights for learning and awareness.
Pingback: How to Deal with Failure: Strategies to Rebuild Confidence