

Introduction
Biological, psychological, and social factors play a major role in shaping our behaviour. One of these is brain chemistry. Dopamine and serotonin are just two of the chemicals in our brain that regulate our thoughts, emotions and behaviours. Dysregulation of these can lead to schizophrenia, bipolar disorder and major depression.
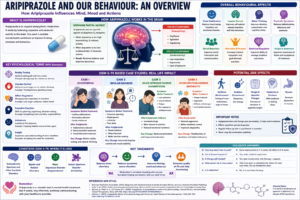
Psychiatrists widely use aripiprazole, an atypical antipsychotic, to correct this imbalance. However other antipsychotics, it not only blocks neurotransmitters, but also modulates them. And its behavioural effects are complex. In this article, we explore some of the ways in which aripiprazole changes behaviour through psychological processes, with examples.
Neurochemical Foundations of Behaviour
To understand how aripiprazole affects behaviour, we must first examine its mechanism of action. Researchers describe aripiprazole as a partial agonist at dopamine D₂ receptors. In psychological and neuroscientific terms, this relates to dopamine regulation, which refers to the balancing of dopamine activity in the brain.
Dopamine influences reward, motivation, pleasure, and reinforcement learning. According to reinforcement theory, rewarding stimuli increase the likelihood that behaviours will be repeated. Excess dopamine activity can lead to heightened salience of irrelevant stimuli, contributing to psychotic symptoms such as hallucinations and delusions. Therefore, low dopamine levels lead to anhedonia, a reduced ability to experience pleasure.
Aripiprazole acts as a stabilizer. In conditions of excess dopamine, it reduces activity, and in conditions of deficiency, it enhances it. This dual action allows for more balanced behavioural responses.
For example, an individual experiencing schizophrenia may interpret neutral events as highly significant due to excess dopamine activity. After treatment with aripiprazole, this misinterpretation often decreases, leading to more reality-based behaviour.
Mood Regulation and Emotional Stability
One of the most significant behavioural effects of aripiprazole is mood stabilization. In psychology, mood refers to a sustained emotional state, while affect regulation describes the ability to manage and respond to emotional experiences appropriately.
In disorders like bipolar disorder, individuals experience mood dysregulation, characterized by alternating episodes of mania and depression. Mania involves elevated mood, impulsivity, and increased goal-directed activity, whereas depression involves sadness, fatigue, and hopelessness.
Aripiprazole helps stabilize these extremes. It reduces manic symptoms such as impulsive decision-making and excessive energy, while also supporting improvements in depressive symptoms when used as augmentation therapy—a term referring to the addition of a second medication to enhance treatment effects.
For instance, a person who previously engaged in risky spending during manic episodes may, after treatment, demonstrate improved impulse control, meaning the ability to delay or inhibit inappropriate actions. This leads to more adaptive and socially acceptable behaviour.
Impulse Control and Executive Function
Another key area influenced by aripiprazole is executive functioning, which includes cognitive processes such as planning, decision-making, and self-regulation. The prefrontal cortex supports executive function and plays a central role in self-control.
Clinicians commonly observe impulsivity—defined as acting without adequate forethought—in mood disorders and certain personality conditions. Aripiprazole helps regulate this by modulating dopamine pathways involved in reward and inhibition.
From a psychological perspective, the concept of delayed gratification explains improved impulse control; it refers to the ability to resist immediate rewards in favour of long-term benefits.
For example, before treatment, an individual might react aggressively in response to minor frustration. After starting aripiprazole, the same individual may pause, evaluate the situation, and choose a more appropriate response. This shift reflects improved executive control over behaviour.
Reduction of Psychotic Symptoms
Aripiprazole is particularly effective in reducing positive symptoms of schizophrenia, such as hallucinations and delusions.
- Hallucinations are perceptual experiences without external stimuli (e.g., hearing voices).
- Delusions refer to fixed false beliefs that resist contrary evidence.
These symptoms reflect distorted reality testing, a psychological concept that describes the inability to distinguish between internal thoughts and external reality.
By regulating dopamine activity, aripiprazole reduces the intensity and frequency of these symptoms. Behaviourally, this results in more coherent speech, reduced paranoia, and improved social interaction.
For example, a person who once believed others were plotting against them may begin to question this belief and interact more openly. This indicates improved reality testing and cognitive flexibility.
Cognitive Functioning and Thought Processes
Cognitive functioning includes attention, memory, and reasoning. Many psychiatric conditions involve cognitive deficits, which can impair daily functioning.
Aripiprazole indirectly improves cognition by reducing symptom severity. This allows individuals to engage more effectively in tasks requiring concentration and problem-solving.
A relevant psychological concept here is cognitive organization, which refers to the ability to structure thoughts logically. In schizophrenia, disorganized thinking may manifest as incoherent speech or difficulty maintaining a topic.
After treatment, individuals often show improved clarity of thought. For example, a person who previously struggled to follow conversations may begin to respond more appropriately and maintain logical continuity.
Social Behaviour and Interpersonal Functioning
Human behaviour is inherently social. Social functioning refers to the ability to interact effectively with others and fulfill social roles.
Psychiatric symptoms often lead to social withdrawal, reduced communication, and impaired relationships. Aripiprazole helps improve social functioning by reducing symptoms such as paranoia, irritability, and emotional instability.
From a psychological standpoint, enhanced theory of mind explains this improvement; it refers to the ability to understand others’ thoughts and emotions.
For instance, a person who previously avoided social interactions due to suspiciousness may begin to participate in conversations and rebuild relationships. This reflects both reduced symptoms and improved social cognition.
Motivation and Reward Processing
The brain’s reward system drives motivation. In psychological terms, goal-directed behaviour refers to actions taken to achieve specific outcomes.
Conditions like depression often involve amotivation and anhedonia. Aripiprazole, by modulating dopamine, can enhance motivation and engagement in activities.
For example, an individual who previously lacked interest in hobbies may gradually resume activities such as reading, working, or socializing. This change reflects improved reward sensitivity and behavioural activation.
Side Effects and Behavioural Implications
While aripiprazole has many benefits, it can also produce side effects that influence behaviour.
One such effect is akathisia, a state of inner restlessness. Psychologically, this reflects a disturbance in psychomotor activity, leading to behaviours such as pacing or an inability to sit still.
Another possible effect is sedation, which may result in reduced activity levels and fatigue. Additionally, changes in appetite and weight can influence self-image and behaviour.
It is important to note that these effects vary among individuals and should be monitored clinically.
Insight and Self-Awareness
Insight is a critical psychological construct referring to an individual’s awareness of their own mental condition. Many psychiatric disorders involve impaired insight, leading to resistance to treatment.
Aripiprazole may improve insight by reducing symptom severity and enhancing cognitive clarity. Behaviourally, this results in greater treatment adherence and more informed decision-making.
For example, a person who previously denied their illness may begin to acknowledge their condition and actively participate in therapy. This marks a significant shift in self-awareness and responsibility.
Long-Term Behavioural Outcomes
Over time, the behavioural effects of aripiprazole can contribute to improved quality of life. Individuals may experience greater emotional stability, better relationships, and increased productivity.
However, it is essential to emphasize that medication alone is not sufficient. According to the biopsychosocial model, effective treatment requires a combination of biological (medication), psychological (therapy), and social (support systems) interventions.
Clinical Applications of Aripiprazole:
A DSM-5-TR Based Psychological and Behavioural Analysis
In contemporary clinical psychology and psychiatry, understanding behaviour requires a structured diagnostic framework. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision provides such a foundation by offering standardized criteria for identifying mental disorders. This framework ensures that diagnosis, treatment planning, and clinical interventions remain consistent and evidence-based.
Among the pharmacological treatments used within this framework, aripiprazole occupies a unique position. Unlike traditional antipsychotics, it functions as a dopamine partial agonist, meaning it stabilizes rather than completely blocks neurotransmitter activity. As a result, its influence on behaviour is not merely suppressive but regulatory—impacting cognition, emotion, and social functioning.
Aripiprazole is commonly prescribed across several DSM-5-TR categories, including schizophrenia spectrum disorders, bipolar disorder, major depressive disorder (as augmentation), and autism spectrum disorder with irritability. Across these conditions, it affects core psychological processes such as reality testing, affect regulation, impulse control, and motivation. The following discussion integrates DSM-based clinical understanding with case illustrations to demonstrate how these behavioural changes occur in real-life contexts.
Schizophrenia: Restoring Reality Testing
Schizophrenia, as defined by DSM-5-TR, is characterized by symptoms such as hallucinations, delusions, disorganized speech, and negative symptoms like diminished emotional expression. At the core of this disorder lies an impairment in reality testing, which refers to the individual’s ability to distinguish between internal thoughts and external reality.
Consider the case of a 24-year-old male who presented with auditory hallucinations and persecutory delusions. He believed that his neighbours were monitoring his activities and frequently reported hearing voices commenting on his behaviour. His social withdrawal further reflected the psychological burden of these symptoms.
From a cognitive perspective, this presentation can be understood through distorted salience attribution, a process in which neutral environmental stimuli are perceived as highly significant or threatening. This distortion is closely linked to excessive dopaminergic activity.
Following treatment with aripiprazole, a gradual but noticeable shift occurred. The intensity of hallucinations reduced, and the conviction in delusional beliefs weakened. Behaviourally, the patient began engaging more in social interactions and demonstrated improved coherence in thought and speech.
This transformation illustrates how aripiprazole facilitates dopamine regulation, leading to improved cognitive organization and restoration of reality testing. Rather than suppressing behaviour, it allows the individual to reinterpret experiences more accurately, thereby promoting adaptive functioning.
Bipolar Disorder: Regulating Mood and Impulsivity
Bipolar I Disorder is marked by episodes of mania, during which individuals experience elevated mood, increased energy, reduced need for sleep, and impulsive behaviour. Psychologically, this reflects severe affective dysregulation and impaired executive control.
A 30-year-old female patient demonstrated classic manic symptoms, including excessive spending, rapid speech, and heightened irritability. Her behaviour showed a clear deficit in impulse control, defined as the inability to delay or inhibit immediate reactions.
After initiating aripiprazole, her symptoms became more manageable. Sleep patterns improved, impulsive behaviours decreased, and her interpersonal relationships stabilized. The medication contributed to restoring affect regulation, enabling her to respond to emotional stimuli in a more balanced manner.
From a psychological standpoint, this improvement also reflects enhanced executive functioning, particularly in decision-making and planning. The patient, who previously made spontaneous financial decisions, began evaluating consequences before acting—demonstrating improved delay of gratification.
Thus, aripiprazole acts as a behavioural stabilizer, reducing extremes without eliminating emotional experience, allowing individuals to function more consistently in daily life.
Major Depressive Disorder: Enhancing Motivation and Reward Processing
Major Depressive Disorder involves persistent low mood, fatigue, feelings of worthlessness, and notably anhedonia, or the inability to experience pleasure. In treatment-resistant cases, aripiprazole is often used as augmentation therapy, enhancing the effects of primary antidepressants.
A 35-year-old male patient exhibited significant motivational deficits. Despite ongoing antidepressant treatment, he remained socially withdrawn and disengaged from daily activities. Psychologically, this reflects behavioural inhibition and reduced reward sensitivity.
After adding aripiprazole, the patient began to show gradual improvement. He reported increased energy, resumed participation in routine activities, and displayed greater emotional responsiveness.
This behavioural shift can be explained through improved dopaminergic functioning, which enhances reward processing and supports behavioural activation—a key concept in cognitive-behavioural therapy. Activities that previously felt meaningless began to regain value, leading to increased engagement with the environment.
In this context, aripiprazole does not simply reduce depressive symptoms; it reactivates the motivational systems necessary for adaptive behaviour.
Autism Spectrum Disorder: Improving Emotional Regulation
Autism Spectrum Disorder is characterized by deficits in social communication and restricted patterns of behaviour. In some individuals, significant irritability and aggression are also present, often due to difficulties in emotional regulation and low frustration tolerance.
A 10-year-old child presented with frequent temper outbursts, aggression toward caregivers, and difficulty adapting to changes in routine. These behaviours reflect challenges in managing emotional responses to environmental stimuli.
With the introduction of aripiprazole, a reduction in aggressive outbursts was observed. The child demonstrated improved emotional control and greater adaptability to changes in routine.
From a psychological perspective, this improvement is linked to stabilization of affect regulation and reduction in reactive aggression, which refers to impulsive responses to perceived frustration or threat. As emotional responses became more regulated, the child was better able to engage in structured behavioural interventions.
Integrating Theory with Clinical Practice
Across these diverse cases, a consistent pattern emerges: aripiprazole influences behaviour through core psychological mechanisms. The biopsychosocial model provides a useful framework for understanding this process. While the medication primarily acts on biological systems (neurotransmitters), its effects extend to psychological functioning (thoughts and emotions) and social behaviour (relationships and interactions).
From a cognitive-behavioural perspective, changes in brain chemistry lead to improved thought patterns, which in turn influence behaviour. For instance, reduced paranoid thinking in schizophrenia leads to increased social engagement, demonstrating the interconnected nature of cognition and behaviour.
Additionally, the concept of neuroplasticity suggests that consistent symptom stabilization may contribute to long-term changes in brain functioning, supporting sustained behavioural improvement.
Ethical and Clinical Considerations
Despite its benefits, the use of aripiprazole must be carefully managed. Individual responses vary, and side effects such as akathisia or sedation may influence behaviour. Ethical practice requires attention to patient autonomy, informed consent, and continuous monitoring.
Medication should always be integrated with psychological and social interventions to ensure holistic care.
Conclusion
Aripiprazole helps regulate brain chemistry—especially dopamine—leading to better emotional stability, impulse control, thinking, and behaviour. Within the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision framework, it is effective across disorders like schizophrenia, bipolar disorder, and depression by reducing symptoms and improving daily functioning.
It does not change personality; it helps restore balance. However, the best results occur when medication is combined with psychological and social support.
Frequently Asked Questions
1. What is Aripiprazole used for?
Aripiprazole is used to treat schizophrenia, bipolar disorder, major depressive disorder (as an add-on), and irritability in autism spectrum disorder.
2. How does aripiprazole affect behaviour?
It regulates dopamine levels, helping improve mood, reduce impulsivity, and stabilize thinking and emotional responses.
3. Does aripiprazole change personality?
No. It does not change personality; it reduces symptoms that interfere with normal behaviour and functioning.
4. What are common psychological effects of aripiprazole?
It improves: Reality testing, Affect regulation, Impulse control, Motivation
5. Can aripiprazole help with depression?
Yes, it is used as augmentation therapy when antidepressants alone are not effective.
6. What is akathisia in aripiprazole?
Akathisia is a side effect involving inner restlessness, where a person feels the need to move constantly.
7. How long does it take to work?
Some effects may appear within 1–2 weeks, but full behavioural improvement can take several weeks.
8. Is aripiprazole safe for long-term use?
Yes, under medical supervision. Regular monitoring is important to manage side effects.
9. Can it improve social behaviour?
Yes, by reducing symptoms like paranoia and mood instability, it can enhance social interaction and communication.
10. Should aripiprazole be stopped suddenly?
No. Sudden discontinuation can cause withdrawal or relapse. Always consult a doctor before stopping.
11. Does it affect motivation?
Yes, it may improve motivation by reducing anhedonia and enhancing reward processing.
12. Is therapy still needed if taking aripiprazole?
Yes. Medication works best when combined with psychotherapy and social support.
References
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. American Psychiatric Publishing.
DeLeon, A., Patel, N. C., & Crismon, M. L. (2004). Aripiprazole: A comprehensive review of its pharmacology, clinical efficacy, and tolerability. Clinical Therapeutics, 26(5), 649–666. https://doi.org/10.1016/S0149-2918(04)90063-1
Stahl, S. M. (2021). Stahl’s essential psychopharmacology: Neuroscientific basis and practical applications (5th ed.). Cambridge University Press.
Burris, K. D., et al. (2002). Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. Journal of Pharmacology and Experimental Therapeutics, 302(1), 381–389. https://doi.org/10.1124/jpet.102.033175
Citrome, L. (2013). Aripiprazole: Review of its pharmacology and clinical use. Expert Review of Neurotherapeutics, 13(5), 537–559. https://doi.org/10.1586/ern.13.42
Meyer, J. M., & Quenzer, L. F. (2018). Psychopharmacology: Drugs, the brain, and behavior (3rd ed.). Sinauer Associates.
Monoprova Counselling, (2026), “Skinner’s Behavioral Theory”, Available at: https://monoprovacounselling.in/skinner-behavioral-theory-operant-conditioning-reinforcement-punishment/
Counselling, (2026), “About Us”,
Monoprova Counselling, (2026), “Contact Us”,
This article is written for knowledge purposes, aiming to help readers understand the topic better and gain useful insights for learning and awareness.