
Panic attacks can be sudden, terrifying surges of fear that peak within minutes and come with pounding heart, breathlessness, dizziness, and a crushing sense of loss of control. Traditional treatments—cognitive behavioral therapy (CBT), breathing retraining, and medications—help many people, but access, cost, stigma, and incomplete response leave room for additional options. Emerging research suggests one promising, low-cost approach: using short bursts of intense physical activity as an in-the-moment intervention to interrupt panic attacks and reduce overall anxiety symptoms. Clinicians and researchers are now investigating how body-based interventions like sprinting, jumping jacks, or high-intensity interval movements might be integrated into psychotherapy to offer rapid, accessible relief.
Why exercise might help during a panic attack
Physiological counteraction:
Panic attacks activate the sympathetic nervous system (fight-or-flight), causing a rapid heart rate, shallow breathing, and adrenaline surge. Short, intense exercise also raises heart rate and breathing, but in a controlled, purposeful way that can shift autonomic balance and redirect bodily sensations from perceived threat to goal-directed movement.
Prediction error and interoceptive recalibration:
When the mind expects catastrophic outcomes based on bodily cues (chest tightness = heart attack), a deliberate physical action that resolves those sensations without harm can generate a “prediction error” — evidence that the feared consequence did not occur. Repeated experiences may recalibrate interoception (internal body-signal interpretation), reducing anxiety sensitivity.
Attention redirection and behavioral activation:
Intense movement demands focus on muscles, rhythm, and effort, interrupting ruminative loops and catastrophic thinking. It also provides immediate behavioral engagement rather than avoidance, which can reduce the learning that bodily sensations equal danger.
Fast endorphin and neuromodulator changes:
Even brief high-intensity bouts can trigger release of endorphins, norepinephrine, and other neuromodulators that influence mood and alertness, potentially reducing anxiety in the short term.
What the research says so far
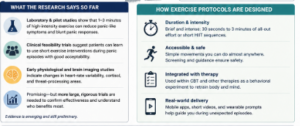
- Laboratory and pilot studies: Early experimental work shows that brief high-intensity exercise (for example, 1–3 minutes of all-out cycling or repeated sprint intervals) can blunt panic-like responses to biological challenge tests (CO2 inhalation) and reduce self-reported panic symptoms immediately afterward. Results vary by protocol and population, but effect sizes are promising enough to justify larger trials.
- Clinical feasibility trials: Small-scale clinical studies and case series suggest patients can learn to use short exercise interventions during panic episodes with good acceptability. Some report rapid symptom reduction comparable to controlled breathing techniques, while others note mild initial discomfort that usually fades with practice.
- Mechanistic investigations: Neuroimaging and physiological studies are exploring changes in heart-rate variability, cortisol, and brain regions involved in threat processing (amygdala, insula). Early data support the idea that exercise changes interoceptive processing and autonomic reactivity, but causal pathways are still being mapped.
How exercise protocols are being designed
- Duration and intensity: Most research focuses on brief (30 seconds–3 minutes) high-intensity bursts or short high-intensity interval training (HIIT) sequences. The key is a rapid shift in effort and breathing rather than prolonged moderate exercise.
- Accessibility and safety: Protocols emphasize movements that are widely accessible (sprinting in place, stair climbs, jumping jacks, burpees) and scalable to fitness level. Safety screening for cardiovascular risk and clear guidance on contraindications are essential.
- Integration with therapy: Clinicians are testing combined approaches—teaching patients to recognize early panic signs, then use an exercise “tool” as a behavioral experiment within CBT frameworks. Therapists help patients plan when and how to use the technique, pair it with cognitive labeling, and process outcomes to reinforce learning.
- Mobile and real-world delivery: Because panic attacks occur unpredictably, studies explore smartphone-guided protocols, short video demonstrations, and wearable-triggered prompts that guide a patient through a brief exercise sequence during an episode.
Potential advantages
- Low cost and scalability: No prescription or special equipment required—most interventions can be learned in a clinic visit and practiced independently.
- Rapid onset of effect: Compared with some therapies or medication onset times, intense exercise can produce near-immediate symptom shifts.
- Empowerment and agency: Active coping strategies can increase patients’ sense of control over panic, countering helplessness and avoidance.
- Complementary to existing treatments: Exercise-based interruptive strategies can augment CBT, exposure work, and breath-based techniques rather than replace them.
Limitations and cautions
- Not universally suitable: People with certain cardiovascular, respiratory, orthopedic, or medical conditions may be unable or unsafe to perform intense exercise. Screening and clinician oversight are necessary.
- Short-term discomfort: Intense activity temporarily raises heart rate and breathlessness—sensations similar to panic—which can be distressing initially. Careful graded exposure and coaching reduce this risk.
- Evidence still emerging: Most studies are small or preliminary. We need larger randomized controlled trials with diverse clinical samples and longer follow-up to determine effectiveness, optimal dosing, and who benefits most.
- Risk of avoidance replacement: If used improperly, exercise could become a safety behavior relied on to avoid fully processing panic in exposure-based therapy. Integration with psychotherapy must prevent reinforcement of avoidance patterns.
Clinical implications and future directions
- Training clinicians: Psychotherapists should be trained in safely assessing fitness and tailoring exercise-based interventions, including when to recommend alternatives.
- Personalized protocols: Research should identify which panic subtypes, comorbidities (e.g., panic disorder with agoraphobia), and individual traits (e.g., baseline fitness, anxiety sensitivity) predict benefit.
- Mechanistic trials: Studies combining physiological monitoring, neuroimaging, and ecological momentary assessment will clarify how exercise changes threat perception and panic trajectories.
- Implementation research: Trials in primary care, community mental health, and low-resource settings will test real-world feasibility, acceptability, and cost-effectiveness.
- Digital augmentation: Smartphone apps, wearables, and brief video coaching may increase reach and provide just-in-time support during panic episodes.

Practical guidance for clinicians and patients (evidence-informed)
- Screen first: Evaluate cardiovascular and musculoskeletal safety and discuss alternatives for medically vulnerable patients.
- Start small and guided: Teach a short, simple sequence (e.g., 30–60 seconds of fast stair stepping or 20–40 seconds of vigorous marching or jumping jacks), practice in session, and debrief.
- Frame as an experiment: Encourage patients to view the exercise as a behavioral experiment to test catastrophic predictions (e.g., “If I push my body briefly, will I lose control?”).
- Combine with CBT skills: Use cognitive labeling (name the panic), grounding statements, and post-exercise processing to reinforce learning and reduce anxiety sensitivity.
- Monitor and adapt: Track outcomes, side effects, and whether the technique reduces avoidance or inadvertently becomes a safety behavior.
Conclusion
Using short bursts of intense physical activity as an on-the-spot intervention for panic attacks offers a promising, low-cost, and scalable complement to established therapies. Early research supports physiological, attentional, and interoceptive mechanisms that could rapidly reduce panic symptoms and reshape fear responses. However, safety screening, cautious protocol design, and robust clinical trials are needed before wide adoption. When integrated thoughtfully into psychotherapy—especially CBT—exercise-based interruptive strategies could empower patients with a practical tool to regain control during panic and help reshape how the body is interpreted in anxiety disorders.
FAQ
1. Can exercise really stop a panic attack?
Short bursts of intense physical activity—like 30–60 seconds of fast stair‑climbing, jumping jacks, or sprinting in place—may help interrupt panic by changing how the body interprets sensations (heartbeat, breath). Early research suggests it can blunt panic symptoms in some people, especially when practiced as part of a broader therapy plan.
2. How does exercise reduce panic symptoms?
Exercise rapidly increases heart rate and breathing in a controlled, purposeful way, which can “override” the body’s panic response. It also shifts attention away from catastrophic thoughts, releases mood‑modulating chemicals (endorphins, norepinephrine), and teaches the brain that intense sensations don’t always mean danger.
3. What kind of exercise is being studied?
Studies focus mainly on brief, high‑intensity bursts (typically 30 seconds to 3 minutes) such as HIIT‑style movements:
- Fast stair climbing
- Jumping jacks or burpees
- Sprinting in place or on a bike
- Repetitive high‑effort movements done in short intervals
4. How quickly does exercise work during a panic attack?
In lab and pilot studies, people often report noticeable symptom reduction within 1–3 minutes of starting a high‑intensity burst. Effects may be similar to controlled breathing or grounding techniques, but individual responses vary.
5. Is this safe for people with panic disorder?
For most otherwise healthy people, short, intense exercise is safe, but medical screening is important. People with heart disease, severe asthma, or other serious conditions should check with a doctor first. Therapy guidance also helps patients avoid turning exercise into an avoidance or “safety‑behavior” trap.
6. Can exercise replace medication or therapy for panic?
No. Exercise is being explored as a low‑cost, in‑the‑moment tool that complements CBT, exposure therapy, and medication, not replaces them. It works best when integrated into a broader treatment plan supervised by a mental‑health professional.
7. Who benefits most from exercise‑based panic interventions?
Early evidence suggests people who:
- Have panic attacks triggered by bodily sensations (chest tightness, racing heart)
- Are physically able to tolerate brief intense effort
- Are willing to practice the technique in and outside therapy
may get the most benefit, but more research is needed.
8. How can someone use exercise safely during a panic attack?
- Start small: 20–30 seconds of brisk marching or jumping jacks, then pause.
- Focus on effort and movement, not “holding back” sensations.
- Practice in therapy first so a clinician can guide pacing and safety.
- Stop and seek help if chest pain, severe dizziness, or faintness occurs.
9. What are the limitations of this approach?
- Evidence is still emerging; most studies are small or preliminary.
- It can feel uncomfortable because the exercise mimics some panic symptoms.
- May not suit everyone, especially those with certain medical conditions or who dread physical exertion.
- It should not become a compulsive safety behavior that replaces processing panic in therapy.
10. How can this be added to existing psychotherapy?
Therapists can:
- Teach the exercise technique in session and normalize the temporary rise in heart rate and breath.
- Use it as a behavioral experiment to test catastrophic beliefs (e.g., “If my heart races, I’ll lose control”).
- Add brief exercise sequences into exposure or in‑vivo panic drills and debrief the outcome to reduce anxiety sensitivity.
Reference
-
Muotri, R. W., Nardi, A. E., de Lacerda, A. L. T., et al. (2026). Brief intermittent intense exercise as interoceptive exposure for panic disorder: A randomized controlled clinical trial. Frontiers in Psychiatry, 17, Article 1739639. Frontiers | Brief intermittent intense exercise as interoceptive exposure for panic disorder: a randomized controlled clinical trial
-
Ströhle, A., Stoy, M., Wiedemann, K., et al. (2005). The acute anxiolytic effect of aerobic exercise in patients with panic disorder. Journal of Psychiatric Research, 39(5), 505–514. – reCAPTCHA
-
Wegner, M., Helmich, I., Machado, S., Nardi, A. E., Arias‑Carrión, O., & Machado, D. (2014). Exercise in the treatment of panic disorder: A systematic review. In Exploring exercise as an avenue for the treatment of anxiety disorders (pp. 1–15). Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2014.00153pubmed.ncbi.nlm.nih+1
-
Broman‑Fulks, J. J., Berman, M. E., Rabian, B. A., & Webster, M. J. (2004). Effects of aerobic exercise on anxiety sensitivity. Behaviour Research and Therapy, 42(2), 125–136. https://doi.org/10.1016/S0005-7967(03)00111-1pubmed.ncbi.nlm.nih
-
Smits, J. A. J., Powell, B. A., & Otto, M. W. (2008). Is exercise a viable treatment for anxiety and panic? Current Psychiatry Reports, 10(4), 265–270. https://doi.org/10.1007/s11920-008-0042-x
- Monoprova Counselling (2026), “About Us”, Available at https://monoprovacounselling.in/
This article is written for knowledge purposes, aiming to help readers understand the topic better and gain useful insights for learning and awareness.